Imagine having your own personal army of cells in your highly advanced defense system, working against outside invaders or abnormal cells where each cell type (over one hundred and eighty-seven recorded) carries their own dedicated function. This specialized team of cells work together to fulfill the complex mission of protecting the body from infection or illness each day.
Our immunity or defense system works in three directives; the first is to (1) RECOGNIZE anything foreign and sound the alarm soon enough to thwart the invader. Molecules and cell surfaces that are identified as foreign are referred to as antigens and have the ability to elicit an immunogenic response. The second function is to (2) RESPOND to the alarm with enough of a counter attack to effectively neutralize the invader quickly. The third directive is to (3) REMEMBER what happened so that if the same situation were to arise again an effective response could be generated faster. The length and efficacy of the immune response depends upon the “intactness” of the underlying biochemistry.
During their lifetime, the cells of the immune system, based upon their experiences and exposures can change their cell surface antigens and their role in the immune response. More than any other organ or system in our body, the immune system is a dynamic system that can change. Like many other cells in our body, the cells of the immune system can be changed from the outside by drugs – Prednisone, Methotrexate, Humira, Remicade, and Plaquenil can suppress the immune system and thus, at least temporarily, help with certain inflammatory diseases, but they don’t heal or redirect the immune response. ............................................................................................................................................................... ENGINEERED KILLER T-CELLS COULD PROVIDE LONG-LASTING IMMUNITY AGAINST CANCER UCLA researchers use stem cells to engineer cells that attack human tumors in mice Sarah C.P. Williams |
They’ve been called the “special forces” of the immune system: invariant natural killer T cells. Although there are relatively few of them in the body, they are more powerful than many other immune cells. In experiments with mice, UCLA researchers have shown they can harness the power of iNKT cells to attack tumor cells and treat cancer. The new method, described in the journal Cell Stem Cell, suppressed the growth of multiple types of human tumors that had been transplanted into the animals. “What’s really exciting is that we can give this treatment just once and it increases the number of iNKT cells to levels that can fight cancer for the lifetime of the animal,” said Lili Yang, a member of the Eli and Edythe Broad Center of Regenerative Medicine and Stem Cell Research at UCLA and the study’s senior author.
Scientists have hypothesized that iNKT cells could be a useful weapon against cancer because it has been shown that they are capable of targeting many types of cancer at once — a difference from most immune cells, which recognize and attack only one particular type of cancer cell at a time. But most people have very low quantities of iNKT cells; less than 0.1% of blood cells are iNKT cells in most cases.
Still, Yang and her colleagues knew that previous clinical studies have shown that cancer patients with naturally higher levels of iNKT cells generally live longer than those with lower levels of cells. “They are very powerful cells but they’re naturally present in such small numbers in the human blood that they usually can’t make a therapeutic difference,” said Yang, who also is a UCLA assistant professor of microbiology, immunology and molecular genetics and a member of the UCLA Jonsson Comprehensive Cancer Center.
Lili Yang, UCLA Broad Stem Cell Research Center
The researchers’ goal was to create a therapy that would permanently boost the body’s ability to naturally produce more iNKT cells. They started with hematopoietic stem cells — cells found in the bone marrow that can duplicate themselves and can become all types of blood and immune cells, including iNKT cells. The researchers genetically engineered the stem cells so that they were programmed to develop into iNKT cells.
They tested the resulting cells, called hematopoietic stem cell-engineered invariant natural killer T cells, or HSC-iNKT cells, on mice with both human bone marrow and human cancers — either multiple myeloma (a blood cancer) or melanoma (a solid tumor cancer) — and studied what happened to the mice’s immune systems, the cancers and the HSC-iNKT cells after they had integrated into the bone marrow. They found that the stem cells differentiated normally into iNKT cells and continued to produce iNKT cells for the rest of the animals’ lives, which was generally about a year. “One advantage of this approach is that it’s a one-time cell therapy that can provide patients with a lifelong supply of iNKT cells,” Yang said.
While mice without the engineered stem cell transplants had nearly undetectable levels of iNKT cells, in those that received engineered stem cell transplants, iNKT cells made up as much as 60% of the immune systems’ total T cell count. Plus, researchers found they could control those numbers by how they engineered the original hematopoietic stem cells. (See complete Press Release in: UCLA Newsroom)
CANCER PREVENTION can be closely aligned with EARLY DETECTION. But from the perspective of a lifestyle upgrade, it is greatly proven that smart nutrition, toxin prevention (smoking, alcohol, drug abuse control), Stress management and Immune system support are all main ingredients to the prevention of cancers. These same protocols, for those who recently underwent cancer treatment, are what medical experts and wellness professionals prescribe to STAY IN REMISSION.
About the Publisher:
JESSE STOFF, MD, HMD, FAAFP - Dr. Stoff is a highly credentialed medical expert specializing in Cancer Immunology and a publisher of current educational programs about Prevention, Wellness and medical texts about Onco-Immunology. As a senior clinical investigator for cancer treatment protocols, Dr. Stoff is dedicated to resolving the most challenging health issues of our time. He has spoken worldwide in some of the top medical conferences about his experiences and analyses on the study of human disease. His medical practice (INTEGRATIVE MEDICINE OF NY, Westbury, NY - www.IMOFNY.com) has been continually providing patients with the many comprehensive clinical options and modalities available- including "ONCO-IMMUNOLOGY", the science of battling cancer cells and reversing pre-cancerous conditions through a complete prevention program that has earned him great success in this field. For more information, visit: www.Dr.JesseStoff.com
DISCLAIMER: All information provided in this article is intended as general public information and is not intended to treat or cure any disease or disorder. NYCRA, nor any individual or practitioner associated with the publishing of this article is not liable for any damages resulting from the use of the information on this article. As a visitor of this blogsite, you acknowledge and agree that any reliance on or use by you of any information available on this Internet web site shall be entirely at your own risk. In no event shall the owner or operator be liable for any direct, indirect, consequential or exemplary damages arising from the use or the performance of this Internet web site, even if the owner or operator has been advised of the possibility of such damages. While every attempt has been made to verify the information on this website, neither the owners, distributors, agents, publishers or their affiliates assume any responsibility or liability for any error, inaccuracies, omissions in the same, or related to results from use of these materials. No party is liable for any direct, incidental, consequential, indirect, or punitive damages arising out of your access to, or use of this blogsite and the contents herein.
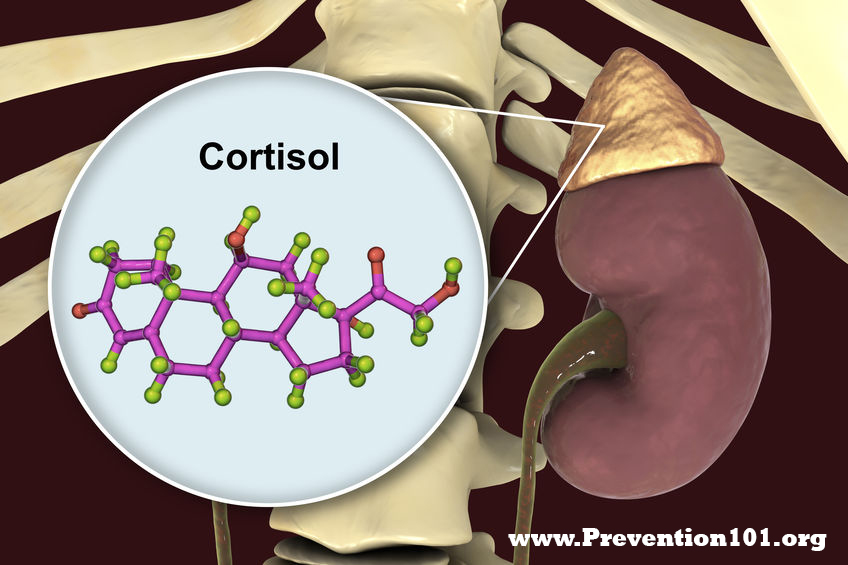
CHRONIC STRESS & HORMONES
The risk of getting cancer is inversely related to the structure and function of the immune system. When the immune system is compromised, then that increases the risk of cancer. Depending upon what's compromising the immune system, that agent or agents can be triggers and/or promoters for the process of cancer itself. Usually that which suppresses the immune system and damages it is also a cancer initiator or promoter. The things that injure the immune system from poor nutrition include zinc deficiencies, Vitamin A deficiency, Vitamin D deficiency etc. Infections like Epstein-Barr, cytomegalovirus, HIV all directly attack cells of the immune system and are oncogenic (viruses that can actually cause and initiate cancer, toxins and certain forms of trauma) specifically x-ray ionizing radiation.
So the way this all fits together comes from the endocrine system - a collection of organs that produce hormones. Hormones are substances that are produced by cell A, that act as some distance away on cell B. So for example, there is a part of the endocrine system called the autonomic nervous system and this is a very important balance in our body, and it's the balance that helps to maintain what's referred to as biochemical homeostasis, the balance between normal biology and fight or flight reactions.
When our body is under stress, and there are many different definitions of stress, one definition that I like is that the capacity to adapt has been exceeded, and the body can no longer compensate for what's going on. Then, the autonomic nervous system will kick in and their short term responsibility to produce substances called catecholamines. These are the fight or flight hormones, epinephrine, norepinephrine, metanephrines, etc. And these will generate a short term response.
When these biochemical substances kick in, they have an effect of stimulating the immune system because in the grand scheme of things, if we are in a fight or flight situation, there's a high risk of injury. And if we are injured, we want the immune system to be up-regulated. They up-regulate the immune system, so that if we get mauled by the saber-toothed tiger, then we can heal from that mauling without dying of septic shock. They're designed for a short term stressor. In our current society, there are plenty of chronic stressors- those that are not time limited to a few seconds or a few minutes, but actually can drag on for hours, days, months, and even years.When the body is under this sort of chronic stress, the body's ability to cope (let it be mental, emotional, physical, physiological) has been exceeded, then the adrenal glands will produce a whole second set of hormones that have the opposite effect. These are cortisol and hydrocortisone. These are the hormones that have an anti-inflammatory effect and have the opposite effect of the catacholamines, and are designed to down-regulate the immune system.
As with everything else in our body, every system has a check and balance in it. If there's an up-regulation response of catacholamines, there's a down-regulation response with the adrenal hormones that are secreted by the cortex, the cortisols and the like, which down-regulate the immune system and are designed to reduce inflammation, which if you're only dealing with a saber- toothed tiger wound, reduces the inflammation and actually speeds the healing process up once the initial immune system has done its response.
As a society, we find people that have a up-regulated cortisol response chronically. And as a result of that, we see a blunting of the normal circadian cycles between cortisol and DHEA. And when this normal cycle is affected because of the chronic secretion of cortisol, what it does is, not only does it down-regulate the immune system, but it's a very important circadian cycle in our body, which affects mood, memory, focus, concentration, menstrual cycles and sleep, amongst many other things, so that when somebody is in a chronic stress, one of the symptoms that they will often complain about is poor sleep, okay? They have trouble falling asleep or trouble staying asleep. They restless this, that, and the other. And that is because this critical circadian cycle has been disrupted.
So the ways of dealing with this are many, but nonetheless the underlying biochemistry is the form of check and balance that the autonomic nervous system has in terms of up-regulating and down-regulating the immune response. Now, when somebody who's into chronic stress, and has high levels of circulating cortisol much longer and much higher than they're supposed to have, and there's production of DHEA is abnormally suppressed, and that of course throws off a whole bunch of other hormones, then that increases their risk of cancer, because the immune system cannot respond the way that it should, because it's being suppressed by the cortisol.
STRESS IS A CANCER PROMOTER
Does the cortisol cause cancer? The answer is at this point, NO. So stress in and of itself biochemically does not cause cancer, but it is certainly a cancer promoter, in that if there is something that will trigger a cancer, and in our environment there's no shortage of things, you just need to have a glass of water, any place in Long Island you're exposed to six different carcinogens. But if you are exposed to something that is a cancer initiator, and your cortisol levels are running high, the immune system is suppressed because of stress, then that will increase the possibility of these abnormal cells that have been triggered by the initiator to progress into a tumor and a full blown cancer. So that's the connection, the way that that works biochemically.
And the biochemistry of all of this is very interesting. There is a direct correlation between stress and cancer, and PTSD and cancer. Though stress and PTSD does not cause cancer, it's that they suppress the immune system, and to the excess and chronic production of cortisol, as a result of the normal stress response that has been exaggerated by the chronic and prolonged stress and PTSD situation. To correct this, if you just go after trying to stimulate the immune system, you're going to have all kinds of wayward reactions and responses because now you have cortisol trying to down-regulate while you're trying to up-regulate, and it's just going to be a traffic jam, and gridlock, and nothing useful is going to happen. So you've got to look at that which is causing stress. So that has to be identified and ameliorated on every level possible that has been identified on.
Blood tests look at cortisol levels. You look at that whole pathway, look at how cholesterol is converted into pregnenolone, converted into DHEA, converted into testosterone, progesterone, estrogen, all the normal hormones and the balance of them, which is the heart of the endocrine system. And you can see, because all of these things would have an effect one way or the other in terms of the stress response and the immune response.
Typically what happens when somebody is in a chronic stress, we see a decrease in their level of pregnenolone or a decrease in the level of DHEA. Often testosterone levels are very low that they're undetectable (yes, women also produce testosterone from their adrenal glands). It happens to be one of the hormones that helps with bone density and osteoporosis. When a woman is under chronic stress, they are exposed to a higher risk of osteoporosis. We conduct blood tests to identify these things, and there are supplements that you can take to balance its deficiency and help the body to reestablish a normal circadian cycle. There is a time to take the cortisol, the hydrocortisone or the DHEA to to effectively and safely support a normal cortisol to DHEA curve.
STRESS & IRREGULAR SLEEP
But a very big piece that people don't pay adequate attention to is all the research that's gone on a circadian cycles looking at the sleep cycle in and of itself, and research has shown very important circadian cycles that kick in from approximately 9:00 at night to 3:00 in the morning, during which time the body can most efficiently repair damage, and the immune system can most efficiently repair itself, and take care of business. But people only go into that restorative cycle if they're actually sleeping, which is why people that work night shifts and swing shifts have a much higher incidence of severe and chronic disease.
There's a whole field of medicine called chronobiology, which would be fat textbooks, I own a couple. But the interesting thing is as they research different circadian cycles that every organ and every system has, it's very ... one of the fascinating things to me is how often the current research that they're doing at Harvard in their Department of Chronobiology, in such places as that, is how often their research about these cycles comes back and shows us the timing of the cycles. And of course, it's local time. The timing is set up by the sun, not by your habit, so that these cycles don't reset themselves, just because we have a habit of going to bed at 3:00 in the morning.
JESSE STOFF, MD, HMD, FAAFP is a highly-credentialed medical expert studying all medical remedies in pursuit of resolving the most challenging health issues of our time. In many circles, he is recognized for his 35+ years of dedicated work in immunology and advanced clinical research in modern CANCER treatments. He has spoken worldwide in some of the most sought-after medical conferences about his experiences and analyses on the study of human disease. His integrative practice (INTEGRATIVE MEDICINE OF NY, Westbury, NY) has been continually providing all patients with the many comprehensive clinical options and modalities available- including "ONCO-IMMUNOLOGY", the science of battling cancer cells and reversing pre-cancerous conditions through a complete prevention program that has earned him great success in this field. visit: www.Dr.JesseStoff.com
Disclaimer & Copyright Notice: The materials provided on this website are copyrighted and the intellectual property of the publishers/producers (The NY Cancer Resource Alliance/IntermediaWorx inc. and Bard Diagnostic Research & Educational Programs). It is provided publicly strictly for informational purposes within non-commercial use and not for purposes of resale, distribution, public display or performance. Unless otherwise indicated on this web based page, sharing, re-posting, re-publishing of this work is strictly prohibited without due permission from the publishers. Also, certain content may be licensed from third-parties. The licenses for some of this Content may contain additional terms. When such Content licenses contain additional terms, we will make these terms available to you on those pages (which his incorporated herein by reference).The publishers/producers of this site and its contents such as videos, graphics, text, and other materials published are not intended to be a substitute for professional medical advice, diagnosis, or treatment. For any questions you may have regarding a medical condition, please always seek the advice of your physician or a qualified health provider. Do not postpone or disregard any professional medical advice over something you may have seen or read on this website. If you think you may have a medical emergency, call your doctor or 9-1-1 immediately. This website does not support, endorse or recommend any specific products, tests, physicians, procedures, treatment opinions or other information that may be mentioned on this site. Referencing any content or information seen or published in this website or shared by other visitors of this website is solely at your own risk. The publishers/producers of this Internet web site reserves the right, at its sole discretion, to modify, disable access to, or discontinue, temporarily or permanently, all or any part of this Internet web site or any information contained thereon without liability or notice to you.
FOREWORD by: Dr. Jesse A. Stoff Recently in the news, they're talking a lot about asbestos and asbestos-related cancers due to 9/11 exposure because when the Twin Towers collapsed, all the asbestos that was in there for insulation was aerosolized. And when you breathe that stuff in, in small particles that have been micronized from the explosion and compression phenomena, when those particles get lodged in the lungs, the body doesn't have a good way to excrete it. Because lung tissue (unlike liver tissue for example) heals by scarring and not regeneration, when the lungs are exposed to chronic irritants that the body can't get rid of, chronic inflammation and irritation ultimately leads to the death of lung cells called pneumocytes. That area of damage causes bronchiectasis and scar tissue formation which can lead to COPD and the diseases associated with that including cardiovascular problems and death. [1] (source: Huntington Patch)
ASTHMA: A MAJOR PREVALENCE WITH FIRST 9/11 RESPONDERS
Fact: no two individuals are ever the same especially when it comes to the physiological effects of envrionmental health hazards- such as those from a disaster zone like Ground Zero. We have all seen countless cases of health issues appearing for the first time 10-15 years after 2001, and the same includes respiratory disorders like ASTHMA.
Where logic may dictate that the giant plume of noxious dust should equate to a widepsread case of pulmonary issues within moments of contact, physicians have observed a variety of effects depending on body types (reflecting genetic makeup) or possibly a unique tolerance level that may actually resist or even 'hide' any symptoms until well past a decade from the exposure. Others may even continue to show zero evidence of negative effects at all (or for now).
"THE TELLTALE COUGH"- EXPLAINED
According to Dr. Paul Schulster, (pulmonologist from Oceanside, NY) the COUGH can say a lot, but often misleads the patient as a "nothing" or a "simple little cough". For firefighters, it is usually a telltale sign of various possible issues. The first syndrome often comes from a post-nasal drip. The second most common cause is from irritation, inflammation and bronchiospasm. Third is Gastroesophageal Reflux Disease. My 9/11-related patients that have GERD starts with that warning cough while others' coughs can trigger the asthma. Finally, Irritative Cough Syndrome can also happen where one cough leads to another cough, irritating the airway, exacerbating another cough - and then another.
Having a cough here or a wheeze there is not enough for most first responders to raise the flag of alarm. Seasoned specialists like Dr. Schulster recognizes that unique and unusual symptoms or maladies do not reach the patient's consciousness for quite some time. Ignoring or not paying more attention to these "little" anomalies tend to often be the norm. These coughs may progressively grow worse over the years and then one day they begin to wheeze a little more than usual and wind up with advancing shortness of breath. Once this becomes significant and finally enters their consciousness, only then will the thought of seeking medical help actually come to mind.
DIAGNOSTIC OPTIONS
Oftentimes, an exam from the pulmonologist starts with the CAT scans of the chest. The firefighters are being tracked for pulmonary nodules. They're referred to as sub-centimeter nodules, which are so small that
you can't read it. "You don't really see them on a plain X-ray, chest X-rays, PA
and lateral. A lot of these first responders already come to me with CAT scans from the past and have been followed by World Trade
Center program and the FDNY doctors that are also pulmonary doctors"- states Dr. Schulster.
In a pulmonologist's tool kit exists certain standard pulmonary function examss- including the SPIROMETRY [2]. This test estimates the narrowing of your bronchial tubes by checking how much air you can exhale after a deep breath and how fast you can breathe out [5]. This allows us to see the best way of determining the lung function in numbers, more or less, is a complete pulmonary function test. Next is the METHACHOLINE CHALLENGE[3] - also known as an asthma trigger that, when inhaled, will cause mild constriction of your airways. If you react to the methacholine, you likely have asthma. This test may be used even if your initial lung function test is normal. [5]Another test used is THE COLD AIR CHALLENGE[4]. The patients generally come with having had those in the past and most are positive for asthma. In the asthmatics.
Inevitably, multiple poisons inhaled in 'the pile' trigger disorders that are obtained on a longterm basis. The isocyanates and the aldehyde may trigger the asthma, "but I'm not certain if we really know the specific cause of their 9/11 based asthma. There's a long list of toxins that irritate and inflame. The probable causes of Asthma are either chronic of acute inflammation. As they breathed in the 9/11 dust, they breathed in 30 of those toxins, causing inflammation in the airways which then led to chronic reactions."
The sub-centimeter nodules seems to be frequent with 9/11 responders. The good news is that most of them turn out to be benign. One follows these nodules for a couple of years with images and CAT scans because they're often too small to really see on plain chest X-rays. And if they remain the same size, they get smaller over a few years, then they're considered benign. And then that's how we deal with it.
Concluding Dr. Schulster's interview, we found that identifying a chronic respiratory disorder like Asthma can be quite involved that there are various diagnostic solutions and treatment options available depending on its classification or severity. Especially in the case of a first responder's long-term exposure to toxic fumes, recognizing the source(s) of contamination can greatly help the physician establish the proper treatment strategy for the patient.
EXTRA: ASTHMA TREATMENT OPTIONS source: https://www.mayoclinic.org/diseases-conditions/asthma/diagnosis-treatment/drc-20369660
Prevention and long-term control are key in stopping asthma attacks before they start. Treatment usually involves learning to recognize your triggers, taking steps to avoid them and tracking your breathing to make sure your daily asthma medications are keeping symptoms under control. In case of an asthma flare-up, you may need to use a quick-relief inhaler, such as albuterol.
Medications
The right medications for you depend on a number of things — your age, symptoms, asthma triggers and what works best to keep your asthma under control. Preventive, long-term control medications reduce the inflammation in your airways that leads to symptoms. Quick-relief inhalers (bronchodilators) quickly open swollen airways that are limiting breathing. In some cases, allergy medications are necessary. Long-term asthma control medications, generally taken daily, are the cornerstone of asthma treatment. These medications keep asthma under control on a day-to-day basis and make it less likely you'll have an asthma attack. See complete list of TREATMENT options and full descriptions @ MAYO CLINIC's website: https://www.mayoclinic.org/diseases-conditions/asthma/diagnosis-treatment/drc-20369660
STAFF EDITOR JESSE STOFF, MD, HMD, FAAFP is a highly-credentialed medical expert studying all medical remedies in pursuit of resolving the most challenging health issues of our time. In many circles, he is recognized for his 35+ years of dedicated work in immunology and advanced clinical research in modern CANCER treatments. He has spoken worldwide in some of the most sought-after medical conferences about his experiences and analyses on the study of human disease. His integrative practice (INTEGRATIVE MEDICINE OF NY, Westbury, NY) has been continually providing all patients with the many comprehensive clinical options and modalities available- including "ONCO-IMMUNOLOGY", the science of battling cancer cells and reversing pre-cancerous conditions through a complete prevention program that has earned him great success in this field. For more information, visit: www.Dr.JesseStoff.com
CONTRIBUTING 9/11 PHOTOGRAPHER KEVIN P. COUGHLIN is a Pulitzer Prize-sharing photojournalist, writer, director of photography, pilot, and aerial cinematographer. He is the current executive photographer to New York Governor Andrew M. Cuomo. His photographs at Ground Zero following the September 11, 2001 attacks on the World Trade Center and while covering funerals and memorial services of fallen fire fighters, police officers, and emergency personnel killed as a result of the attacks are included in the 2002 Pulitzer Prize awarded to The New York Times for Public Service. In addition to The New York Times, his photographs have appeared in the New York Post, New York Daily News, Newsday, The Philadelphia Inquirer, https://www.kevincoughlinphotography.com/
PROFESSIONAL INTERVIEWED IN THIS ARTICLE
PAUL L. SCHULSTER, MD PC is a practicing Pulmonary Disease Specialist in Oceanside, NY. Dr. Schulster graduated from University of Kentucky College of Medicine in 1972 and has been in practice for 47 years. He completed a residency at Queens Hospital Center. Dr. Schulster also specializes in Internal Medicine. Dr. Schulster also practices at South Nassau Community Hospital. One Healthy Way Oceanside NY. His private practice is located at: 442 Waukena Avenue, Oceanside, New York. 11572 | (516) 599-8234
Disclaimer & Copyright Notice: The materials provided on this website are copyrighted and the intellectual property of the publishers/producers (The NY Cancer Resource Alliance/IntermediaWorx inc. and Bard Diagnostic Research & Educational Programs). It is provided publicly strictly for informational purposes within non-commercial use and not for purposes of resale, distribution, public display or performance. Unless otherwise indicated on this web based page, sharing, re-posting, re-publishing of this work is strictly prohibited without due permission from the publishers. Also, certain content may be licensed from third-parties. The licenses for some of this Content may contain additional terms. When such Content licenses contain additional terms, we will make these terms available to you on those pages (which his incorporated herein by reference).The publishers/producers of this site and its contents such as videos, graphics, text, and other materials published are not intended to be a substitute for professional medical advice, diagnosis, or treatment. For any questions you may have regarding a medical condition, please always seek the advice of your physician or a qualified health provider. Do not postpone or disregard any professional medical advice over something you may have seen or read on this website. If you think you may have a medical emergency, call your doctor or 9-1-1 immediately. This website does not support, endorse or recommend any specific products, tests, physicians, procedures, treatment opinions or other information that may be mentioned on this site. Referencing any content or information seen or published in this website or shared by other visitors of this website is solely at your own risk. The publishers/producers of this Internet web site reserves the right, at its sole discretion, to modify, disable access to, or discontinue, temporarily or permanently, all or any part of this Internet web site or any information contained thereon without liability or notice to you.
There are many types of cancer treatments. The types of treatment that you have will depend on the type of cancer you have and how advanced it is. Some people with cancer will have only one treatment. But most people have a combination of treatments, such as surgery with chemotherapy and/or radiation therapy. You may also have immunotherapy, targeted therapy, or hormone therapy.
Clinical trials might also be an option for you. Clinical trials are research studies that involve people. Understanding what they are and how they work can help you decide if taking part in a trial is a good option for you.
When you need treatment for cancer, you have a lot to learn and think about. It is normal to feel overwhelmed and confused. But, talking with your doctor and learning all you can about all your treatment options, including clinical trials, can help you make a decision you feel good about. Our Questions to Ask Your Doctor About Treatment may help.
Surgery: When used to treat cancer, surgery is a procedure in which a surgeon removes cancer from your body. Learn the different ways that surgery is used against cancer and what you can expect before, during, and after surgery.
Radiation Therapy: is a type of cancer treatment that uses high doses of radiation to kill cancer cells and shrink tumors. Learn about the types of radiation, why side effects happen, which ones you might have, and more.
Chemotherapy: is a type of cancer treatment that uses drugs to kill cancer cells. Learn how chemotherapy works against cancer, why it causes side effects, and how it is used with other cancer treatments.
Immunotherapy to Treat Cancer- helps your immune system fight cancer. Get information about the types of immunotherapy and what you can expect during treatment.
Targeted Therapy is a type of cancer treatment that targets the changes in cancer cells that help them grow, divide, and spread. Learn how targeted therapy works against cancer and about common side effects that may occur.
Hormone Therapy is a treatment that slows or stops the growth of breast and prostate cancers that use hormones to grow. Learn about the types of hormone therapy and side effects that may happen.
Stem Cell Transplants are procedures that restore blood-forming stem cells in cancer patients who have had theirs destroyed by very high doses of chemotherapy or radiation therapy. Learn about the types of transplants, side effects that may occur, and how stem cell transplants are used in cancer treatment.
Precision Medicine helps doctors select treatments that are most likely to help patients based on a genetic understanding of their disease. Learn about the role precision medicine plays in cancer treatment, including how genetic changes in a person's cancer are identified and used to select treatments.
Disclaimer & Copyright Notice: The materials provided on this website are copyrighted and the intellectual property of the publishers/producers (The NY Cancer Resource Alliance/IntermediaWorx inc. and Bard Diagnostic Research & Educational Programs). It is provided publicly strictly for informational purposes within non-commercial use and not for purposes of resale, distribution, public display or performance. Unless otherwise indicated on this web based page, sharing, re-posting, re-publishing of this work is strictly prohibited without due permission from the publishers. Also, certain content may be licensed from third-parties. The licenses for some of this Content may contain additional terms. When such Content licenses contain additional terms, we will make these terms available to you on those pages (which his incorporated herein by reference).The publishers/producers of this site and its contents such as videos, graphics, text, and other materials published are not intended to be a substitute for professional medical advice, diagnosis, or treatment. For any questions you may have regarding a medical condition, please always seek the advice of your physician or a qualified health provider. Do not postpone or disregard any professional medical advice over something you may have seen or read on this website. If you think you may have a medical emergency, call your doctor or 9-1-1 immediately. This website does not support, endorse or recommend any specific products, tests, physicians, procedures, treatment opinions or other information that may be mentioned on this site. Referencing any content or information seen or published in this website or shared by other visitors of this website is solely at your own risk. The publishers/producers of this Internet web site reserves the right, at its sole discretion, to modify, disable access to, or discontinue, temporarily or permanently, all or any part of this Internet web site or any information contained thereon without liability or notice to you.
DR. MANU JAIN, Optical Imaging Specialist at Memorial Sloan
Kettering Cancer Centre (MSKCC) Department of Dermatology provides great
insight on the advantages of Reflectance Confocal Microscopy (RCM) for the
diagnosis of skin cancers, in vivo.
RCM is a form of in vivo microscopy— “histopathology-like”
diagnosis without doing a biopsy. It
offers several advantages over conventional light microscopy, including imaging
of tissue in vivo and ability to provide bedside diagnosis. In addition to its
applications in dermatology it can also be applied for oral cancers. Meanwhile, we call this application ‘optical
biopsy’. Microscopy is actually what's
paving the way for digital imaging in dermatology. Before this it was the naked
eye and magnifying lens.
THE POWER OF LIGHT
As ultrasound is recognized for being non-invasive and
radiation free, so is optical imaging – gathering cellular and nuclear
epidermal and superficial dermal information through the use of LIGHT and
laser.It penetrates the skin to reach an
estimated 200 micron in depth - good enough in dermatology to diagnose skin
cancers like melanoma, basal cell carcinoma, and squamous cell carcinoma.
Because most tumors that appear originates at the dermo-epidermal junction
(around a hundred-micron depth from skin surface). In addition to morphological
and cellular details, RCM also provides
information on the dynamic phenomenon of the
blood flow very clearly.
Dr. Jain joined MSK four years ago, but this technology has
been used primarily for researchprior
to her joining in the USA. The engineering team at MSK (headed by Dr. Milind Rajadhyaksha) helped design this machine in
collaboration with Caliber ID (Rochester, NY) 20+ years ago.Few years ago, RCM acquired a category I current
procedural terminology (CPT) reimbursement codes
(96931–96936) by the US Centers for Medicare and Medicaid Services (CMS) [1]. However,
there are limited expert readers of RCM in the US. To bridge this gap, Dr. Jain
teaches and trains her residents in the dermatology and dermatopathology. She
is has started her own annual CME accredited confocal courses at Memorial Sloan
Kettering Cancer Center. She is also the Vice-president of recently formed
American Confocal Group.
This innovation relies solely on reflectiveness of various
tissue structures in the skin, illuminating and magnifying images by relying on
the light planes. “Your skin is like a mirror and when you shine light on the
mirror, whatever absorbs all the light becomes dark and whatever reflects all
the light appears bright”.
"I think it could be interesting to explore the option
of combining confocal microscopy with ultrasound because ultrasound can give us
the doppler information and also the depth is a very good with ultrasound…
which we miss with confocal microscopy.So that would be really great. Like they have done with confocal and
optical coherence tomography."
Her professional
focus is to teach RCM to dermatologists and dermatopathologists.For the large institutions, it’s fairly
affordable and cost-effective as it takes only 15 minutes or 20 minutes to do
one lesion.That means a patient gets
scanned and diagnosed at the same time. This saves a lot of time for the
patient at the end of the day because the patient doesn't have to wait for the
biopsy report for week.
According to Dr. Jain's original bedside diagnosis study,,
RCM has shown remarkable sensitivity (~90%) and specificity (~70%) in hands of
a novice, within a short interval of 16 months [2] , for skin cancers..Several studies reported RCM imaging to
achieve sensitivity of 70–92% and specificity 84–88% for melanocytic lesions
[3] and sensitivity of 100–92% and specificity 85–97% for non-melanocytic skin
lesions . . "As an example, we’re examining a patient's new mole with
confocal microscopy and if we are suspicious that it might be melanoma, we can
use dermoscopy and confocal together to improve the accuracy of diagnosis.
Although the sensitivity of RCM has not much changed over
dermoscopy but the specificity is two times superior—translating into marked
decrease in benign biopsies.
RCM TECHNOLOGY DEVELOPMENT
Thanks to the developmental expertise of Dr. Milind
Rajadhyaksha (member of the faculty of Memorial Sloan Kettering Cancer Center),
the IN VIVO CONFOCAL MICROSCOPY is fast becoming the new standard in dermal
non-invasive imaging.Originally
conceptualized with his mentors at MD Anderson (renowned physicist Dr. Robert
Webb and dermatologist/laser pioneer Dr. Rox Anderson), the team sought better
ways to detect skin cancers while reducing the need for biopsies in real time
at the bed-side.At the time, biopsy and
pathology were the standard approach for detecting and diagnosing skin
lesions.The demand for advancing
diagnostic imaging was a call from the 5 million+ new cases diagnosed in the US
each year and another million cases detected in Europe, UK, Australia, other
regions of the world.
Milind (as he prefers to be called) described how the RCM
works in simplified terms: “We start with a bright light source… in our case
it's a laser.We focus the laser down to
a very tiny spot inside the skin and we move the spot around in 2 dimensions so
we create essentially a plane of illumination by moving that spot. Imagine
having a flashlight which you point at a wall and now you move the flashlight
back and forth, sideways and up and down until you can illuminate the entire
wall.Similarly, we ‘paint’ a single
plane within tissue with focused laser spot and we collect light from each
location that the spot illuminates and that we can use that to produce an
image. You can essentially create an image or a picture of a single layer of
cells or layer of tissue within skin.”
Milind states having built the original laboratory bench top
portion in the early 1990’s and continued the expansion of the technology with
MSKCC since 2005. He has been involved with advancing both the IN vivo (means
directly on the patient) and the EX vivo microscope (referring to any fresh
tissue that has been removed from the patient, ie. biopsy) to do faster imaging
over large areas. Besides looking at skin cancers, this technology is set up
over a mic top with a probe that can allow for imaging inside the oral cavity
looking for oral cancers. “We've done a lot of work in imaging to guide
treatment, surgeries and to guide laser ablations at Memorial for more than a
decade.”
Disclaimer & Copyright Notice: The materials provided on this website are copyrighted and the intellectual property of the publishers/producers (The NY Cancer Resource Alliance/IntermediaWorx inc. and Bard Diagnostic Research & Educational Programs). It is provided publicly strictly for informational purposes within non-commercial use and not for purposes of resale, distribution, public display or performance. Unless otherwise indicated on this web based page, sharing, re-posting, re-publishing of this work is strictly prohibited without due permission from the publishers. Also, certain content may be licensed from third-parties. The licenses for some of this Content may contain additional terms. When such Content licenses contain additional terms, we will make these terms available to you on those pages (which his incorporated herein by reference).The publishers/producers of this site and its contents such as videos, graphics, text, and other materials published are not intended to be a substitute for professional medical advice, diagnosis, or treatment. For any questions you may have regarding a medical condition, please always seek the advice of your physician or a qualified health provider. Do not postpone or disregard any professional medical advice over something you may have seen or read on this website. If you think you may have a medical emergency, call your doctor or 9-1-1 immediately. This website does not support, endorse or recommend any specific products, tests, physicians, procedures, treatment opinions or other information that may be mentioned on this site. Referencing any content or information seen or published in this website or shared by other visitors of this website is solely at your own risk. The publishers/producers of this Internet web site reserves the right, at its sole discretion, to modify, disable access to, or discontinue, temporarily or permanently, all or any part of this Internet web site or any information contained thereon without liability or notice to you.
FOREWORD By Dr. Robert L. Bard, cancer diagnostic specialist (NYC) After a decade past the 9/11 disaster, news broke of unique and advanced cases of CANCER arising in droves. A growing number of the same individuals exposed to the toxic fumes and plumes of hazardous particles in the danger zone have recently contracted aggressive cases of CANCER and were in immediate demand for medical care and desperate need for advanced research and support. This spike in cases can only come from ‘dormant’ cells or recurrence (usually with a vengeance) – such as cases of cancer tumors in the lung, liver, prostate, kidney, brain, skin and even the eye. To troubleshoot each case, it would be advantageous to take a crash course in toxicology and to recognize the chemical compounds that BATHED all responders during the event. Understanding these chemicals can help us pursue their behaviors (on the body) and their long and short term effects.
TOXICOLOGY 101: A THREAT TO FIREFIGHTERS HEALTH
As part of our evaluation of all occupational illnesses contracted by first responders, we enter the world of TOXICOLOGY- the branch of science focused on the effects and detection of poisons. It is also the discipline overlapping chemistry, biology and pharmacology- studying the adverse effects of chemical substances on living organisms. In pursuit of first responders’ safety as far as chemical effects on the body, we connected with Professor David Purser of the Hartford Environmental Research (UK), a renowned toxicology expert who conducted major reviews on fire-exposed carcinogens published worldwide. “9/11 was unusual in that a major environmental hazard resulted from the dust cloud released as and after the Towers collapsed,” says Prof. Purser. “The dust inhaled by responders at the time, and afterwards working at the site, has resulted in serious ongoing and developing health conditions and to this day.
For fires in general, there is also increasing evidence and concern regarding FF exposure to carcinogens, especially from soot contamination to skin and clothing following attendance at incidents and during training.” An abstract from Prof. Purser’s latest presentation – “ Toxins Including Effects of Fire Retardants, During Fires and Post-Fire Investigation Activities” indicates a remarkable breakdown of some of the major toxins and carcinogenic compounds that the average firefighter would be exposed to.
Below is a list of common toxic elements found in active fires and post-fire investigations that first responders have been known to be exposed to.
•PARTICULATES: especially ultrafine particles + metals
These toxins are usually found within active fire zones- either inside the fire event itself or downwind plume in the form of residues and soot or lethal fragments activated at high temperatures or in airborne smoke. These asphyxiant gases, irritants and particulates are the main causes of injury and death of fire victims exposed to high concentrations inside burning buildings. Asphyxiant gases cause collapse with loss of consciousness during a fire, leading to death if exposure continues. Irritants and smoke particulates cause pain to the eyes and lungs, with breathing difficulties, which inhibit escape during a fire and can lead to lung inflammation and edema within a few hours of rescue, which can also be fatal. Those surviving may make a good recovery or suffer long term neurological or cardio-respiratory health effects, depending on the severity of the exposure. Those most at risk from these effects at the fire scene are building occupants and emergency responders not protected by breathing apparatus.
Beyond the immediate fire zone, especially outside a burning building, or during wildfires, these toxic smoke products are considerably diluted by mixing with outside air, so are generally not immediately life-threatening. The main hazards to unprotected persons exposed to the diluted smoke plume in the surrounding area are health risks from inhalation of smoke irritants and soot particulates, or from inhalation of mineral particles and fibers. The immediate effects of exposure are mainly eye and throat irritation, with a sore throat and cough in some cases over a period of a few days, although persons with pre-existing respiratory or circulatory health conditions may be more severely affected. Longer term health hazards following a single exposure may result from inhalation of sensitizers (such as isocyanates or formaldehyde), which can cause asthma, or from some mineral dusts and fibers, which may remain in the lungs. Health risks from exposure to carcinogens during a single incident are generally low, although the World Trade Center dust and some chemical fires may be exceptions.
Health risks to firefighters result mainly from repeated exposures to inhalation of smoke toxicants and contact with soot deposits. These contain a wide variety of carcinogens, so that cumulative exposure over years may present an increased cancer risk. The hazards arise from inhalation of smoke, soot or mineral fibers, but also from soot contamination of skin or clothing. This can result in dermal, inhalation or oral ingestion, resulting in increased exposure to carcinogens, including dioxins and dibenzofurans, during post-fire activities. Halogenated fire retardants (especially chlorine and bromine systems), present possible increased health risks to fire victims and firefigthers during fires due to inhibition of combustion in the vapor phase resulting in inefficient combustion with an increase in yields of toxic carbon and nitrogen compounds, in addition to the formation of acid gases, dioxins and dibenzofurans under all fire conditions..**
“IT ALL STARTS
AT THE LUNGS" Historical Patterns of Carcinogenic Reactions from Environmental Disasters by: Dr. Jesse Stoff
If you review the victims of a disaster such as the radioactive fallout in CHERNOBYL, then compare it to the dust from the 911 catastrophe, you can find a similar behavior as far as how fatalities come to appear within a certain timeline. There’s the initial contamination that results in immediate illnesses- and then there’s a major wave of cancer cases that arise a decade later. These cancers are delineated on the CDC website and are occurring, undoubtedly, because of the mixture of toxins that people have been exposed to. The volume of these toxins are absorbed into their bodies since 9/11 (while working with the clean-up efforts) and can't get rid of them.
We are seeing patients with very unusual blood borne cancers that have had very unusual genetic profiles -undoubtedly because of the unusual combination of carcinogenic toxins that people were exposed to that have been lingering in their system for so many years. We're also seeing a marked increase in Monoclonal Gammopathies (MGUS) and Myelofibrosis which is progressive damage to the bone marrow that itself can become a cancerous process. We're seeing many people suffering changes to the structure and functioning of their immune system even without yet developing a cancer but for those kinds of changes their risk of developing skyrockets. Also, because of the shifting in their immune system we see a significant increase in the level of different kinds of allergies (including environmental based) that have become more prevalent and worse than before the exposure to this kind of toxic material.
In essence, the destruction and suffering continues.
THE KILLER DUST
by Capt. Richard
Marrone (9/11 Responder)
"It was just
everywhere. The DUST was so thick it would dry your eyes out. You couldn't
breathe. As EMS, that was a lot of what we were doing was just constantly
cleaning people's eyes out. There's nothing you can do to get away from it. I
know what was in those particulates--it was asbestos, it was concrete, it was
human remains, metals and any possible contamination in a fire... it was all
there. Nobody was protected. Even the firefighters who had self-contained
breathing apparatus, you're only getting 15 or 20 minutes maximum on those
cylinders, and there just wasn't enough to keep constantly replacing them. The
police officers and EMS personnel were using surgical masks, which basically
provided no protection whatsoever. We
mostly treated rescue workers on site due to the dust-- eyes and stuff like
that. There really wasn't enough eye or respiratory protection, so anybody
that became a patient post-collapse was due to the contamination and the
toxins of 9/11."
RESPONDERS PULMONOLOGY REVIEW Following the logical path of carcinogen, one would start from how environmental contaminants would make their way into the body; through the respiratory ports. As seen in the toxicology section of this article, these foreign substances range from particulates like metals and acids to microfragments to molecular-sized compounds whose behaviors vary from mild irritants to lethal poisons. More often than not, these compounds can trigger cell mutations in our physiology as well as attack our very immune system to penetrate our defenses for tumors to grow.
Our responders’ health report brought us to interview Pulmonary and Sleep Medicine Specialist Dr. Mayank Shukla (NYC) who helped identify the various diagnostics and screening procedures for first responders often start with a Pulmonary Function Test to study a patient’s airway size, and then a Bronchodilator Challenge Test to identify and distinguish between asthma and COPD. Another protocol for patients exposed to airborne contaminants is examining airway resistance and looking for Upper Airway Resistance Syndrome (UARS), Sleep Apnea and other breathing disorders caused by an impairment of the airway size.
The concern for the responder’s air passage brings telltale signs of possible impending issues based on their condition that brings warning signs of what may lie ahead- in the lungs, the bloodstream etc. There's another test which is available called NIOX designed for a patient to have allergy component or asthma that also is very sensitive, to look at the lung inflammation for these patients. During airway inflammation, higher-than-normal levels of nitric oxide (NO) are released from epithelial cells of the bronchial wall. 4 The concentration of NO in exhaled breath, or fractional exhaled nitric oxide (FeNO), can help identify allergic/eosinophilic inflammation, and thereby support a diagnosis of asthma when other objective evidence is lacking. (See NIOX.com)
There are other testing available which helps us to do a direct visualization of the upper and lower levels. For example, there's the bronchoscopy for the lungs and air passages and then there's the laryngoscopy to visualize the nasal cavity, the sinus, sinusitis, the larynx, because many of these patients have acute or chronic laryngitis because getting exposed to the several toxins. Also, many of them have gastro esophageal reflux, so when you look at that endoscopy, you can realize that this patient have, you know, chronic inflammation of the, not only for a lower airway, but also with upper airway as well.
Disclaimer & Copyright Notice: The materials provided on this website are copyrighted and the intellectual property of the publishers/producers (The NY Cancer Resource Alliance/IntermediaWorx inc. and Bard Diagnostic Research & Educational Programs). It is provided publicly strictly for informational purposes within non-commercial use and not for purposes of resale, distribution, public display or performance. Unless otherwise indicated on this web based page, sharing, re-posting, re-publishing of this work is strictly prohibited without due permission from the publishers. Also, certain content may be licensed from third-parties. The licenses for some of this Content may contain additional terms. When such Content licenses contain additional terms, we will make these terms available to you on those pages (which his incorporated herein by reference).The publishers/producers of this site and its contents such as videos, graphics, text, and other materials published are not intended to be a substitute for professional medical advice, diagnosis, or treatment. For any questions you may have regarding a medical condition, please always seek the advice of your physician or a qualified health provider. Do not postpone or disregard any professional medical advice over something you may have seen or read on this website. If you think you may have a medical emergency, call your doctor or 9-1-1 immediately. This website does not support, endorse or recommend any specific products, tests, physicians, procedures, treatment opinions or other information that may be mentioned on this site. Referencing any content or information seen or published in this website or shared by other visitors of this website is solely at your own risk. The publishers/producers of this Internet web site reserves the right, at its sole discretion, to modify, disable access to, or discontinue, temporarily or permanently, all or any part of this Internet web site or any information contained thereon without liability or notice to you.





 JESSE STOFF, MD, HMD, FAAFP - Dr. Stoff is a highly credentialed medical expert specializing in Cancer Immunology and a publisher of current educational programs about Prevention, Wellness and medical texts about Onco-Immunology. As a senior clinical investigator for cancer treatment protocols, Dr. Stoff is dedicated to resolving the most challenging health issues of our time. He has spoken worldwide in some of the top medical conferences about his experiences and analyses on the study of human disease. His medical practice (INTEGRATIVE MEDICINE OF NY, Westbury, NY - www.IMOFNY.com) has been continually providing patients with the many comprehensive clinical options and modalities available- including "ONCO-IMMUNOLOGY", the science of battling cancer cells and reversing pre-cancerous conditions through a complete prevention program that has earned him great success in this field. For more information, visit: www.Dr.JesseStoff.com
JESSE STOFF, MD, HMD, FAAFP - Dr. Stoff is a highly credentialed medical expert specializing in Cancer Immunology and a publisher of current educational programs about Prevention, Wellness and medical texts about Onco-Immunology. As a senior clinical investigator for cancer treatment protocols, Dr. Stoff is dedicated to resolving the most challenging health issues of our time. He has spoken worldwide in some of the top medical conferences about his experiences and analyses on the study of human disease. His medical practice (INTEGRATIVE MEDICINE OF NY, Westbury, NY - www.IMOFNY.com) has been continually providing patients with the many comprehensive clinical options and modalities available- including "ONCO-IMMUNOLOGY", the science of battling cancer cells and reversing pre-cancerous conditions through a complete prevention program that has earned him great success in this field. For more information, visit: www.Dr.JesseStoff.com
























{kind=link}