
Introduction by: Dr. Robert L. Bard, MD, PC, DABR, FASLMS

This program was yet another proof that DIGITAL ULTRASOUND is the future of emergent diagnostics. What makes ultrasound a perfect device for this remote diagnostic paradigm is its ability to come in many PORTABLE models. Also, ultrasound is fast responding, safe (radiation free), non-invasive and easy to learn with a trainer. This is the perfect formula for satisfying the many critical care situations where the reality of distance can be addressed with technology.
THE DIAGNOSTIC OVERREADER: YOUR VIRTUAL RADIOLOGIST
The concept of REMOTE imaging has been around for decades. My practice has been involved with some of the most complex clinical trials and treatment partnerships with hospitals in Italy, Australia, Germany and other foreign lands, reviewing, investigating or confirming scans like MRI's, CT and Ultrasound. To operate high-powered imaging technology is a craft in and of itself, but to READ what you see, then to dig deeper to 'play detective' and to drive the investigative process with accuracy and intuition is a solid contribution to any medical team.
 |
| Click to see complete Remote Self-Screening Program |
Thanks to the advancements of our web-based communication tools, overseas collaboration via electronic FILE-SHARING has been streamlined to empower and facilitate the world of patient care. As with TELEMEDICINE (where a patient and physician's time and safety are better supported) the concept of installing a Radiological Overreader in any patient care facility is part of our next generation of unified medicine.
BENEFITS OF AN IMAGING OVERREADER PARTNERSHIP:
1) Installing an affordable value added service to any practice
2) A second opinion is PEACE OF MIND of all your scans from a certified Radiologist- adding new diagnostic support to your patients
3) Expands your ability to collaborate with other physicians as well as treating your patients remotely
4) Having advanced imaging analysis reduces the level of RISK by raising a level of validity and added confidence to all your medical reports relating to complex scans
5) As a virtual partnership, having an overreader is an affordable upgrade to your staff without the overhead
 |
| D2D: Doctor-to-Doctor is a common term in TeleMed Conferencing uniting physicians in active sites (Point of Care activity with patient) + a remotely accessed medical radiologist placed on the scene via WIFI. |
...................................................................................................................................................................
OVERREADING IN CLINICAL TRIALS
Diagnostic Imaging in Remote Team Research Studies
From product testing to quality reviews of treatment solutions and medicines, proposed innovations undergo intensive assessment protocols to achieve the highest possible levels of quantitative data-gathering necessary- and to prove the EFFICACY of any product. To pass all the strict regulatory guidelines for public distribution, testing labs are the last line of defense for public health and safety by either confirming or rejecting manufacturers' claims. SAFETY is the other top consideration in product reviews- ensuring the low-to-zero level of risk from public use. Once a product in question has fulfilled the initial staging guidelines of testing, a means to confirm effectiveness and safety (on humans) is through CLNICAL TRIALS where a population of patients is monitored for any and all biochemical effects. Forms of scanning and detection include observational surveying, blood & skin testing, mechanical stress-testing, bio-simulations and the use of clinical imaging technologies (when applicable). Innovations like advanced ultrasound is a common option for repeat checking of any bodily responses. Today's sonograms are preferred by primary investigators for their fast, accurate and affordable data collecting. In addition, repeat use for tracking and monitoring is completely safe (non-radiation) for any patient.
 "Before & After" Studies
"Before & After" Studies
The most sensible and logical way to identify the results of any treatment is by tracking the body's response to it. Controlled testing must show the patient's condition PRE and POST effects, where true data-finding is collecting the necessary EVIDENCE of its claims. The investigator can pull a significant amount of data from this form of scan-testing: including stage-by-stage bodily response to future projections of possible side effects. Recording of any and all psysiological response means the researchers are counting on the patient's body to tell us what it is undergoing during the testing phase. To prevent mis-reading and erroneous reports, trials tend to work with a large number of test patients (commonly 50-100) and may also employ redundancies like undergoing multiple testing protocols for a second or even third opinion. To capture the benefits of a BEFORE AND AFTER review, Imaging is often used as a standard screening solution for the response of most of the major organs.
WHAT ARE B LINES? Expert ultrasound readers are trained to identify anomalies in organ performance. In the case of screening for possible Covid-related pathogen response, B-lines are often sought after as a prime indicator of fluid in the lungs. They can be visualized as hyperechoic vertical lines extending from the pleura to the edge of the ultrasound screen. These lines are sharply defined and laser-like and they typically do not fade as they progress down the screen. A few B-lines that move along with the sliding pleura can be seen in normal lung due to acoustic impedance differences between water and air. However, excessive B-lines are abnormal and are typically indicative of underlying lung pathology.
...................................................................................................................................................................

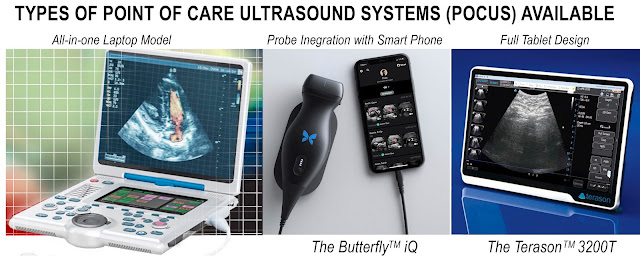
GOING PORTABLE: Fast Response for Field Demands
Once upon a time, ultrasound imaging device design were large and cumbersome, often the size of a refrigerator. They were one-piece units with wheels to support in-hospital traveling. But over time, as the medical community took to the ultrasound as the reliable choice for quick, accurate scanning, so did the demand to scan patients out on the field. From ambulances, cruise ships, commercial airlines and even the space program, the design of the ultrasound steered toward more PORTABLE, and HAND-HELD models.
The battery-powered, pocket-sized ultrasound machine became commercially available in the late 1990s where smaller and lighter devices with higher image quality such as those manufactured by GE Healthcare, Siemens and Philips dominated this portable market. These pocket-sized ultrasound machines allowed clinicians to have immediate visual correlation with physical examination findings. They also allow for quick and instant assessments, which are extremely important for emergency physicians. At a healthcare resource allocation level, they significantly reduce a patient’s waiting time and improve clinician’s workflow. Furthermore, the cost of pocket-sized ultrasound machines is much lower than that of standard ones. [3]
A recent study from emergent care physicians and EMT's have called on the need for "pre-hospital imaging"- where the need for efficiency in applying "precious seconds" of focused care means everything. Portable scanners and handheld ultrasound devices are clearly expanding toward at-home versions all the way to “battlefield” models called “the modern stethoscope”- today’s solution to fast, initial examinations and real-time response, timely suited for our current health crisis and beyond.

A recent study from emergent care physicians and EMT's have called on the need for "pre-hospital imaging"- where the need for efficiency in applying "precious seconds" of focused care means everything. Portable scanners and handheld ultrasound devices are clearly expanding toward at-home versions all the way to “battlefield” models called “the modern stethoscope”- today’s solution to fast, initial examinations and real-time response, timely suited for our current health crisis and beyond.
Contributors & Technical Advisors

ROBERT L. BARD, MD, PC, DABR, FASLMS
Advanced Imaging & Diagnostic Specialist
Dr. Bard received the 2020 nationally acclaimed Ellis Island Award for his lifetime achievement in advanced cancer diagnostic imaging. He co-founded the 9/11 CancerScan program to bring additional diagnostic support to all first responders from Ground Zero. His main practice in midtown, NYC (Bard Diagnostic Imaging- www.CancerScan.com) uses the latest in digital imaging technology and has been also used to help guide biopsies and in many cases, even replicate much of the same reports of a clinical invasive biopsy. Imaging solutions such as high-powered sonograms, Power Doppler Histogram, sonofluoroscopy, 3D/4D image reconstruction and the Power Doppler Histogram are safe, noninvasive, and do not use ionizing radiation.
 PIERRE KORY, M.D., M.P.A.
PIERRE KORY, M.D., M.P.A.
Dr. Kory is Board Certified in Internal Medicine, Critical Care, and Pulmonary Medicine. He served as the Medical Director of the Trauma and Life Support Center at the University of Wisconsin where he was an Associate Professor and the Chief of the Critical Care Service. He is considered a pioneer and national/international expert in the field of Critical Care Ultrasound and is the senior editor of the widely read textbook “Point-of-Care Ultrasound” (winner of the President’s Choice Award for Medical Textbooks from the British Medical Association in 2015). Most recently, Dr. Kory joined the emergency volunteer team during the early COVID-19 pandemic in NYC at Mount Sinai Beth Israel Medical Center. He is also a founding member of the Front Line COVID-19 Critical Working Group (flccc.net) composed of 5 critical care experts that devised the COVID-19 treatment protocol called MATH+. (www.covid19criticalcare.com/)
 MICHAEL THURY, RDCS, RVT, FASE
Michael is the current Global Product Manager for Terason Ultrasound (Burlington, MA). Commercially he has spent the last 19 years training physicians, clinicians and distribution partners around the world on the uses and benefits of ultrasound. He has been recognized numerous times for outstanding clinical and sales excellence both at Terason and GE Healthcare. Michael holds a AAS in Cardiovascular Technology from Southeast Technical College and is a South Dakota native. https://www.terason.com/
MICHAEL THURY, RDCS, RVT, FASE
Michael is the current Global Product Manager for Terason Ultrasound (Burlington, MA). Commercially he has spent the last 19 years training physicians, clinicians and distribution partners around the world on the uses and benefits of ultrasound. He has been recognized numerous times for outstanding clinical and sales excellence both at Terason and GE Healthcare. Michael holds a AAS in Cardiovascular Technology from Southeast Technical College and is a South Dakota native. https://www.terason.com/
PIERRE KORY, M.D., M.P.A.Dr. Kory is Board Certified in Internal Medicine, Critical Care, and Pulmonary Medicine. He served as the Medical Director of the Trauma and Life Support Center at the University of Wisconsin where he was an Associate Professor and the Chief of the Critical Care Service. He is considered a pioneer and national/international expert in the field of Critical Care Ultrasound and is the senior editor of the widely read textbook “Point-of-Care Ultrasound” (winner of the President’s Choice Award for Medical Textbooks from the British Medical Association in 2015). Most recently, Dr. Kory joined the emergency volunteer team during the early COVID-19 pandemic in NYC at Mount Sinai Beth Israel Medical Center. He is also a founding member of the Front Line COVID-19 Critical Working Group (flccc.net) composed of 5 critical care experts that devised the COVID-19 treatment protocol called MATH+. (www.covid19criticalcare.com/)
MICHAEL THURY, RDCS, RVT, FASE



























{kind=link}