
Collaborative Action Behind COVID-19 Tools R&D supported by The UN Foundation
By: Rachel Bridges- Senior Global Health Advocacy and Communications Manager for the United Nations Foundation | Edited by: Prevention101.org
"The COVID-19 pandemic has demonstrated the interconnected nature of our world – and that no one is safe until everyone is safe. Only by acting in solidarity can communities save lives and overcome the devastating socio-economic impacts of the virus. In partnership with the United Nations, people around the world are showing acts of humanity, inspiring hope for a better future." - The United Nations, We’re All in This Together.
 |
| Photo credit: Institut Pasteur (courtesy of the UN Foundation) |
While research developments are still in early stages, we are seeing the fastest R&D efforts in human history unfold. Through WHO’s leadership, a genetic sequence of the novel coronavirus (COVID-19)—a previously unknown disease—was shared with the world just 2 weeks after its initial discovery. Through coordinated efforts led by WHO, research and development is rapidly moving forward so that everyone, everywhere can have access to tools to help prevent, detect, and respond to COVID-19. Some examples of these efforts include:
- WHO’s global Solidarity Trial aims to rapidly develop an effective treatment for COVID-19. As of mid-August 2020, the Solidarity Trial has more than 3500 patients enrolled with more than 100 countries participating, including more than 400 hospitals in 35 countries alone. According to the WHO, the Solidarity Trial will reduce the amount of time it normally takes for a drug trial to determine effectiveness by 80%. This, combined with the size and geographic breadth of the trial, will provide a strong evidentiary basis behind specific therapies that can then be acted upon quickly by health systems.
 |
| Photo credit: University of Queensland (courtesy of the UN Foundation) |
- WHO has published a research and development roadmap, with a set of protocols for how studies should be done to create potential therapeutics or vaccines.
- WHO is already working with scientists across the globe on over 120 different candidate vaccines for coronavirus with eight already in clinical trials in record time — just a few months after sequencing the gene.
- 10 vaccine candidates in clinical evaluation and 123 in pre-clinical evaluation
 |
| Photo credit: UNICEF |
The UN Foundation helps support COVID-19 treatment research through mobilizing resources via the COVID-19 Solidarity Response Fund, as well as supporting WHO and partners working to discover COVID-19 treatments through advocacy and communications efforts with policy makers, global funders, and the general public. We help share scientific information as its being discovered, as well as advocate for continued investments in this critical research and development efforts being coordinated by WHO and global partners like UNITAID, the Global Fund, and others through the ACT Accelerator.
WHO plays a critical role in coordinating a range of global health initiatives, including the global response to COVID-19. To this point, it has served as the global coordinator of efforts to develop vaccines, tests and treatments; trained millions of health workers; distributed millions in medical supplies, while also continuing the fight against other major health threats that matter to Americans like malaria, measles, and HIV/AIDS.
Currently, WHO’s efforts and the global COVID-19 response are undergoing challenges due to political challenges between member states. However, WHO’s global scientific research initiatives continue to forge ahead toward its imperative to resolve the pandemic. Only though coordinated and collaborative action can we stop this virus for everyone, everywhere. To help support WHO and partners’ global COVID-19 response, visit the COVID-19 Solidarity Response Fund website.
Currently, WHO’s efforts and the global COVID-19 response are undergoing challenges due to political challenges between member states. However, WHO’s global scientific research initiatives continue to forge ahead toward its imperative to resolve the pandemic. Only though coordinated and collaborative action can we stop this virus for everyone, everywhere. To help support WHO and partners’ global COVID-19 response, visit the COVID-19 Solidarity Response Fund website.
ABOUT THE AUTHOR:


Feb. 27, 2021 - Health providers and educators at the European Pandemic front and Cancer Care societies, in support of global information sharing- aligned with NYCRA-NEWS, expressing complete support of a global health initiative. NYCRA-TV is forming international partnerships and alliances starting with our first Italian translated video of our top NYC cancer diagnostic expert Dr. Robert Bard with this trailer from his 2021 presentation on cancer diagnostic innovations. (SEE video clip). "This is the start of a collaborative union between countries to exchange information from our respected fields... and drive an inspired bond, presenting the best of what a global coalition of caregivers and scientists can bring!"- states a representative of the upcoming program "Notizei Globali- IT (Global Health News) "

SCIENTIFIC ALLIANCES: UNITED MINDS ON A COMMON MISSION
This pandemic has clearly illustrated that "Scientists by nature do not see borders or politics - only solutions", states Dr. Robert Bard, cancer diagnostics expert (NYC). "The spirit of teamwork is alive and well with this community- especially in a crisis. Historically, medical and scientific people have always raced to the front lines - always at the ready to pool resources and collaborate. Like the domestic and international health associations, we continue to see some of the sharpest clinical minds in the world- including American teams that are now coming out with promising protocols to help end this pandemic. To contain and eliminate this human threat means UNITING WITH SCIENCE AND WORKING TOGETHER ON A COORDINATED GOAL." Such is the case with this remarkable grouping of like minds under a targeted objective. They call themselves The Front Line Covid-19 Critical Care Alliance - highly published critical care specialists from major academic medical centers with collectively over 1,000 medical publications. Meet Some of the "Top Medical Minds in the Front Lines"  (Founding members & clinical advisors of MATH+ formed The Front Line Covid-19 Critical Care Alliance). (Founding members & clinical advisors of MATH+ formed The Front Line Covid-19 Critical Care Alliance).Based on the rapidly emerging research into COVID-19, the early clinical experience in China reflected by the Shanghai expert commission, and their decades-long clinical and research experiences in severe infectious diseases around the country, the 5 experts developed the MATH+ Hospital Treatment Protocol for Covid-19. It is intended for use early in the hospitalization of patients presenting with states of respiratory distress requiring supplemental oxygen. These 5 have since been joined by an increasing number of hospitalist and ICU physicians who recognize the sound physiologic rationale, the emerging published research in support of the components, and the data demonstrating good clinical outcomes in hospitals that have adopted the treatment regimen. 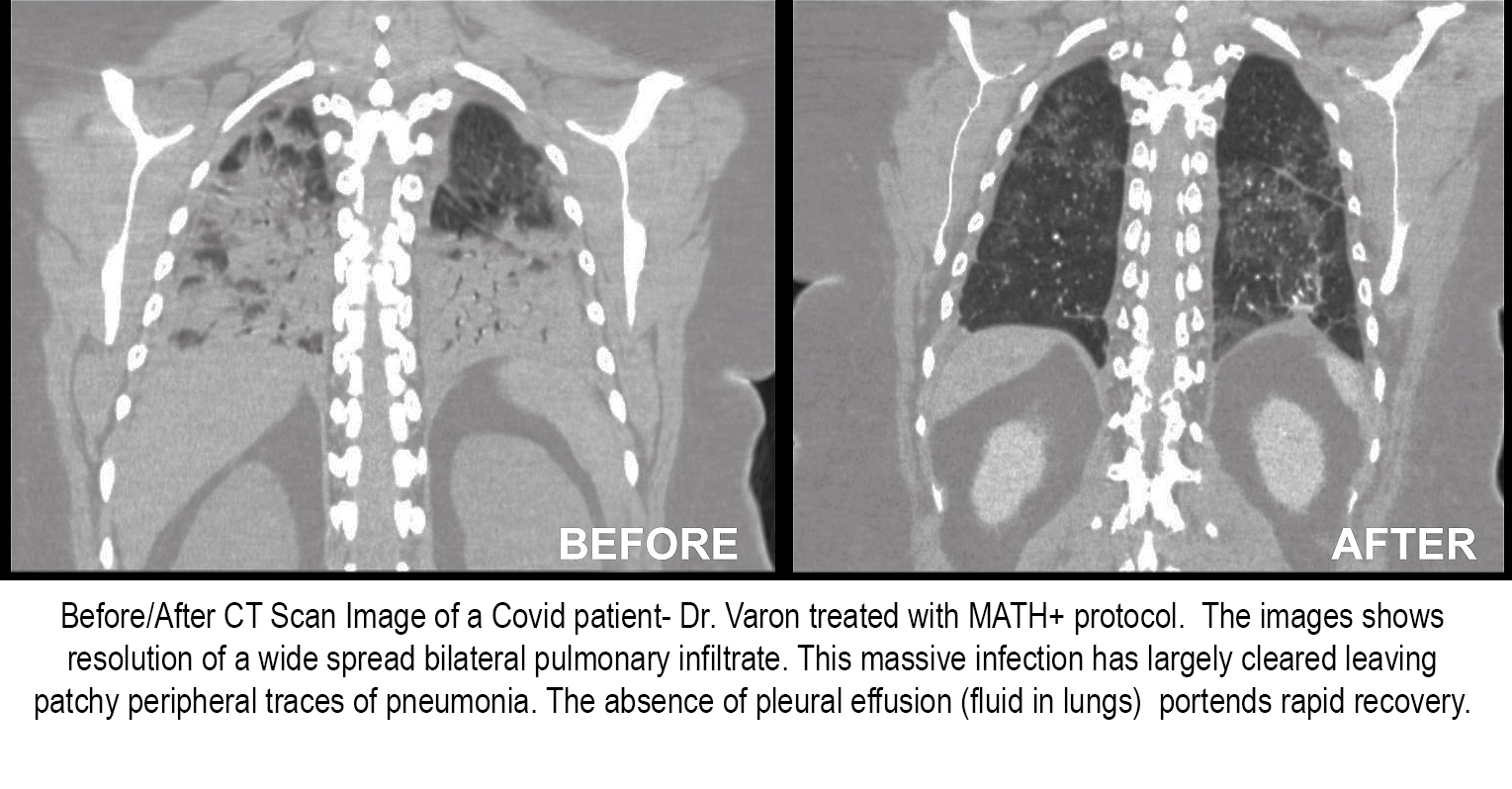 Methylprednisolone & MATH+: Treatment Success Data from the Nation's "HOT SPOTS" Methylprednisolone & MATH+: Treatment Success Data from the Nation's "HOT SPOTS"With a confirmed global count of 9.27+ Million cases and 470,000+ deaths, the world continues its desperate search for a treatment that will save the lives of COVID-19 patients who come into the ER or hospital with low oxygen levels or struggling to breathe. Where the more popular treatment for patients in ICU is the use of ventilators, a reported 80-85% of Covid-19 patients on ventilators in New York end up dying (Associated Press and state and city officials).  The corticosteroid Methylprednisolone is a key component, based on large studies that have proven its effectiveness in prior viral pandemics‐ and whose potency is significantly increased when administered intravenously with high doses of the antioxidant Ascorbic acid (Vitamin C). Thiamine (Vitamin B1) is given to optimize cellular oxygen utilization and energy consumption, protecting the heart, brain, and immune system and the anticoagulant Heparin prevents (or breaks up) blood clots that increasingly appear as illness worsens. The + represents other supportive treatments by the administering doctor for patients who present other pre‐existing conditions (as needed). The group also plans to add or change components and dosing as published medical literature evolves. The corticosteroid Methylprednisolone is a key component, based on large studies that have proven its effectiveness in prior viral pandemics‐ and whose potency is significantly increased when administered intravenously with high doses of the antioxidant Ascorbic acid (Vitamin C). Thiamine (Vitamin B1) is given to optimize cellular oxygen utilization and energy consumption, protecting the heart, brain, and immune system and the anticoagulant Heparin prevents (or breaks up) blood clots that increasingly appear as illness worsens. The + represents other supportive treatments by the administering doctor for patients who present other pre‐existing conditions (as needed). The group also plans to add or change components and dosing as published medical literature evolves.LATEST UPDATES: According to physicians implementing the MATH+ Covid-19 treatment protocol, conclusive data shows significant success by as much as 97%, where only 3-6.6% mortality- from hospital reports including the VIRGINIA DEPT. OF HEALTH. (See complete report) See LINK for complete "ESSENTIALS on MATH+ Covid-19 intervention protocols" |

"MATH+ Saved my Life"- patient story
VIEWPOINTS

As soon as SARS-CoV-2 began generating international
attention, I knew that the scientific community would rally. After working in a
virus research lab for 3 years, I know that science and passion often go hand
in hand. Collaboration is at the heart of research, especially successful
research but it is also notoriously a slow and methodical process. Rushed
science is often flawed, which is why peer-review and open access is so
critical. … We live in historical times and pandemics set the stage for
innovation (e.g. Solidarity Trial and Solidarity Response Fund). Most vaccine
technology is the product of many years of hard work. International emergencies
have a way of opening the peoples' eyes to fields that typically operate away
from the worlds eyes (e.g. research, public health, Infection Control).
| EPILOGUE: Epidemiology
By: Lennard M. Gettz & Cheri Ambrose/ NY Cancer Resource Alliance
 June 24, 2020- Months into the CoronaVirus pandemic, the tally of efforts expended by government health agencies and professionals worldwide has been noted to significantly exceed any global campaign in history. Economists tend to use war terms to help put the pandemic's containment efforts and collateral damage in perspective. IMF's chief economist Gita Gopinath, (in an April 15 news conference) stated that "the best case scenario, the world is likely to lose a cumulative $9 trillion in output over two years"- making this a global war 3x the fiscal size of World War II. June 24, 2020- Months into the CoronaVirus pandemic, the tally of efforts expended by government health agencies and professionals worldwide has been noted to significantly exceed any global campaign in history. Economists tend to use war terms to help put the pandemic's containment efforts and collateral damage in perspective. IMF's chief economist Gita Gopinath, (in an April 15 news conference) stated that "the best case scenario, the world is likely to lose a cumulative $9 trillion in output over two years"- making this a global war 3x the fiscal size of World War II.
As with past wars, alliances were formed, industries were committed to task and scientists worldwide have united by sharing information toward this single directive. The Department of Global Communications (U.N.) announced their drive to mobilize global cooperation in science-based COVID-19 responses, "The United Nations is mobilizing international cooperation to harness the power of science to tackle the coronavirus pandemic, while also working with partners to explore innovative crisis response tools."
Unlike the early months of the year, the second quarter showed the front lines to finally "catching up to the war efforts" with installments of these comprehensive containment measures:
|
Other articles recently published in Prevention101.org

Source: MD Anderson Cancer Center
Watch how a blacklight reveals what improper hand washing can leave behind. According to Dr. Christina Le-Short of MD Anderson Cancer Center, "Cancer patients are at greater risk of developing complications from respiratory viruses... Effective hand-washing is your best defense against germs that cause the flu or Covid-19".

Source: NIOSH SCIENCE BLOG
Reports about Prolonged PPE Use by healthcare workers are aligned with health issues from abnormally elevated carbon dioxide (CO2) levels in the blood causing increased pressure inside the skull, nervous system changes, cardiovascular effects and reduced tolerance to lighter workloads that may lead to possible dizziness, hyperventilation and dehydration. View the report by the CDC about the many physiological effects of breathing increased concentrations of CO2 and the effects of failing overused respirator masks: See complete article
 Suggested Safety Measures for Covid Prevention in Medical Offices From respirators to hand sanitizers to regular use of hospital-grade disinfectants, the medical community is trusted to apply and set standards when it comes to safety measures, risk prevention strategies and sanitizing efforts. This new article offers a collective set of smart and sensible safety ideas from a group of doctors in your area. Promoting SAFETY GUIDELINES in any health practice is everyone's duty in our community. See complete article
Suggested Safety Measures for Covid Prevention in Medical Offices From respirators to hand sanitizers to regular use of hospital-grade disinfectants, the medical community is trusted to apply and set standards when it comes to safety measures, risk prevention strategies and sanitizing efforts. This new article offers a collective set of smart and sensible safety ideas from a group of doctors in your area. Promoting SAFETY GUIDELINES in any health practice is everyone's duty in our community. See complete articleReferences:
1) Some doctors moving away from ventilators for virus patients: https://apnews.com/8ccd325c2be9bf454c2128dcb7bd616d
2) Global economy to be worst hit since Great Depression: Gita Gopinath, Chief Economist, IMF
3) W.H.O. CASE COUNT: https://covid19.who.int/?gclid=CjwKCAjw88v3BRBFEiwApwLevVNWB8VzRXQYzS6KGVe1QkdIdQ7P5G4SoXNIeYnTSKcIooGXKqbIzBoCnIkQAvD_BwE
4) UChicago Medicine doctors see 'truly remarkable' success using ventilator alternatives to treat COVID-19 https://www.uchicagomedicine.org/forefront/coronavirus-disease-covid-19/uchicago-medicine-doctors-see-truly-remarkable-success-using-ventilator-alternatives-to-treat-covid19
5) Ventilators: Helping or Harming COVID-19 Patients https://www.webmd.com/lung/news/20200415/ventilators-helping-or-harming-covid-19-patients#1
6) Study: 88% of coronavirus patients on ventilators died in NY
7) Coronavirus patients on ventilators are unusually likely to die, causing some doctors to change strategy
8) Texas Medical Center Data: https://www.tmc.edu/
9) Nearly 9 in 10 COVID-19 patients who are put on a ventilator die, New York hospital data suggests
10) Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area
11) Center for American Progress: Removing Barriers for Immigrant Medical Professionals Is Critical To Help Fight Coronavirus https://www.americanprogress.org/issues/immigration/news/2020/04/02/482574/removing-barriers-immigrant-medical-professionals-critical-help-fight-coronavirus/
12) UN Foundation: HOW THE WORLD’S SCIENTISTS, DOCTORS, AND NURSES ARE UNITING TO FIGHT COVID-19 https://unfoundation.org/blog/post/how-worlds-scientists-doctors-and-nurses-uniting-fight-covid-19/
Disclaimer & Copyright Notice: The materials provided on this website are copyrighted and the intellectual property of the publishers/producers (The NY Cancer Resource Alliance/IntermediaWorx inc. and Bard Diagnostic Research & Educational Programs). It is provided publicly strictly for informational purposes within non-commercial use and not for purposes of resale, distribution, public display or performance. Unless otherwise indicated on this web based page, sharing, re-posting, re-publishing of this work is strictly prohibited without due permission from the publishers. Also, certain content may be licensed from third-parties. The licenses for some of this Content may contain additional terms. When such Content licenses contain additional terms, we will make these terms available to you on those pages (which his incorporated herein by reference).The publishers/producers of this site and its contents such as videos, graphics, text, and other materials published are not intended to be a substitute for professional medical advice, diagnosis, or treatment. For any questions you may have regarding a medical condition, please always seek the advice of your physician or a qualified health provider. Do not postpone or disregard any professional medical advice over something you may have seen or read on this website. If you think you may have a medical emergency, call your doctor or 9-1-1 immediately. This website does not support, endorse or recommend any specific products, tests, physicians, procedures, treatment opinions or other information that may be mentioned on this site. Referencing any content or information seen or published in this website or shared by other visitors of this website is solely at your own risk. The publishers/producers of this Internet web site reserves the right, at its sole discretion, to modify, disable access to, or discontinue, temporarily or permanently, all or any part of this Internet web site or any information contained thereon without liability or notice to you.
©Copyright Intermedia Worx Inc./Prevention 101. All Rights Reserved.
























{kind=link}