From an interview with Maty Torres, BHSc, RVT
In our ongoing study of non-invasive diagnostic modalities, we connected with Chief Vascular Technologist & Technical Director of
Cooperman Barnabas Medical Center's (CBMC) Non-Invasive Vascular Lab, Ms. Maty Torres. Her vast experience on the use of the Transcranial Doppler provided extensive insight on its many advantages in patient care for both Radiology and Vascular units.
As a career technologist, Ms. Torres started in vascular sonography (1990) then received her first exposure to the field of TCD scanning 1998. In the early part of her tenure, she performed Transcranial Doppler Imaging on a patient population from the Valerie Fund Children’s Center (A NJ based non-profit group providing support for the comprehensive health care of children with Cancer and blood disorders) for pediatric sickle cell patients. By 2011 her expertise with cerebral doppler scanning were called to new challenges.
As a team-supporting service, Ms. Torres advanced to the next stage of TCD utility in non-imaging TCD exam where this protocol provided great data-gathering advantages in emergent and post-surgical cases for medical collaboration between residents and neuro specialists by monitoring subarachnoid hemorrhage patients for new onsets of vasospasm in Neuro ICU cases. She expresses the major LEARNING CURVE behind being proficient at operating TCD scanning. "This is not a test that you could cross train in a short period and perform it adequately. Without an image for guidance, you are using audible sounds, waveforms, and direction of flow, thus relying on the technologist’s expertise to find the correct arteries. I have seasoned technologists that range from 11 to 20 years of experience in the field; however, only few perform this study because it’s very specific.”

Ms. Torres adds, “When a patient is admitted with a subarachnoid hemorrhage, the goal is to search for the source. Some patients might require Endovascular Coiling (treatment to block blood flow/bleeding throughout the body) and recover in the Neuro ICU. We support the neuro team by providing scheduled monitoring by daily TCD’s evaluating increases in ratios that could detect an increased risk of an onset of vasospasm."
Her facility currently uses the Nicolet® SONARA® TCD system. While these hospital-grade devices can be used for Emboli detection or interoperate scanning for PFO (Patent Foramen Ovale) closures, Ms. Torres' current assignments are primarily focused on neuro-monitoring for the detection of increased risks of vasospasms. As a seasoned technical expert in various levels of TCD field use, Ms. Torres shares field insight on the medical applications of this diagnostic protocol. "I see an opportunity to use TCD for patients with symptomatic carotid stenosis at our facility.”
SPECIAL TRAININGHer training on TCD imaging first started in 2001 with an intensive training course presented by Medical College of Georgia School of Medicine led by
Dr. Robert J. Adams currently at the Medical University of South Carolina working directly on Sickle Cell patients. Dr. Adams is considered a pioneer in using transcranial doppler (TCD) and transcranial Doppler imaging (TCDi) to assess stroke risk in children with sickle cell anemia (SCA). He also helped discover that regular blood transfusions can reduce strokes by as much as 90 percent in these children.[4] Additional training came from Natus training experts who come from many areas such as the
Swedish Institute of Neurology and a comprehensive text:
Practical Guide to Transcranial Doppler Examinations by Dr. Andrei Alexandrov.
Maty Torres, BHSc, RVT, Chief Vascular Technologist/Technical Director, Non-Invasive Vascular Lab. Seasoned Vascular Technologist with a demonstrated history of working in the hospital and health care industry. Skilled in Vascular Sonography, Data Analytics, Health Informatics, and Peer Mentoring. Strong information technology professional with a B.H.Sc. focused in Health Care Administration from Nova Southeastern University, currently pursuing a Master’s in Business Administration from William Patterson University.
REFERENCES:
2) https://pubmed.ncbi.nlm.nih.gov/1926257/
THE SCIENCE OF BLOOD FLOW AND DOPPLER TECHNOLOGY
Hemodynamics is defined as the study of blood flow in relation to the status of the circulatory system and homeostatic mechanisms of autoregulation. Through the monitoring of blood flow, diagnostic analysis can provide many answers to the health and physiological status of the target area scanned as well as cell-level metabolism, the regulation of the pH, osmotic pressure and temperature of the whole body, and the protection from microbial and mechanical harm.[1] Assessing injuries, inflammation or mutative growths (like cancer tumors), assessment of blood flow provides diagnostic answers about the severity of tissue disorders or tumor malignancy.
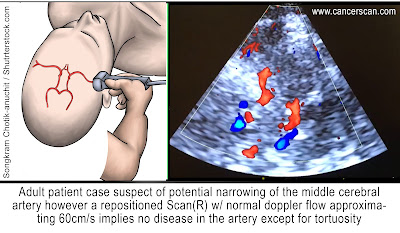
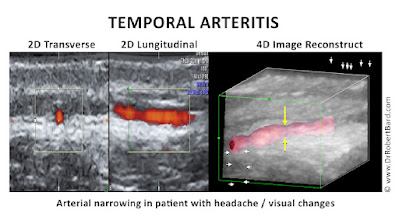
The expansion of ultrasound research and development broke new ground in 1982 when Dr. Rune Aaslid (Norwegian Neurosurgical researcher) first introduced Cerebral Hemodynamics with the implementation of Transcranial Doppler science to offer noninvasive transcranial recorded imaging of flow velocity in basal cerebral arteries. His report detailed that placing an accurately configured Doppler ultrasound transducer in the temporal area (just above the zygomatic arch)offers quantitative data of the blood flow velocity in the middle, proximal anterior and posterior cerebral arteries.[1.2] This scan is critical for detecting vasospasms and for reviewing circulation in the brain for potential disease of the carotid and vertebral arteries. [1.5]

In 1989, Dr. Aaslid published the first study on dynamic cerebral autoregulation in humans - a biological and metabolic function dedicated to stabilizing cerebral blood flow. TCD detects the slightest change in perfusion-- the volumetric measure at which blood is delivered to tissue, or volume of blood per unit time per unit tissue mass. Alongside the study of blood pressure, Cerebral Autoregulation is vital to maintaining life as it supports proper delivery of adequate oxygen (in the blood) and nutrients to the brain and the removal of CO2 & other waste products.[2] As Dr Aaslid used the TCD by scanning through the transtemporal approach, others explored the intracranial arteries through the orbital (eye socket) window. By the early 90's, the next generation of development teams (Spencer, Seidel, Dobson & Moehring) improved on the Doppler innovation to detect microemboli and hemodynamic physiology. Today, TCD is widely accepted and utilized for an expanding set of clinical and research applications including ischemic stroke, sickle cell disease, subarachnoid hemorrhage and vasospasm.
According to cancer diagnostic imaging expert Dr. Robert Bard, the introduction of 4D Doppler technology aligned with the ultrasound's base design concept of providing instantaneous, real time readings. "Let's take the case of breast cancer screening, the technician simply puts the probe on the breast, finds the area, pinpoints it, presses a button and seconds later you have the map showing the types of vessels, volumetric arterial density and spatial location of the vessels in relation to the adjacent organs. You have functions that give you a vessel density measurement which shows how aggressive this is. Instead of genetic markers (which are very popular), visually displaying tumor aggression performed in a matter of seconds to show cancer vessel invasion is a game-changer for any early detection or monitoring facility. Tumor aggression by blood flow evaluation is used worldwide in nuclear medicine, CT scans and MRI technology, however, one of the simplest and most cost-effective alternatives is the non‐invasive 3D Doppler breast procedure."
INTRACRANIAL SCANNING WITH DOPPLER ULTRASOUND
In 1982, continued advancement led to the Transcranial Doppler (TCD) ultrasonography for outpatient and inpatient settings. By integrating the ability to study BLOOD FLOW into a low-frequency transducer, placing the probe on the temporal area measures the cerebral arteries to detect and quantify cerebrovascular activities, diseases and brain injuries. Other applications include the diagnoses of vasospasm (VSP) after an aneurysm rupture, hemorrhage or hemodynamic changes after ischemic or cryptogenic stroke. It also enables the study of cranial pressure fluctuations. TCD also offers significant clinical benefits in the monitoring of sickle-cell disease by scanning brain stem death and elevated raised intracranial pressure (ICP). Added features allow for surgical and post-op monitoring of vasomotor functions as well as detecting critical disorders like a microembolism.
SUMMARY OF TARGET CONDITIONS FOR TCD APPLICATIONS
• Vasospasm /aneurysm
• Sickle cell anemia, to determine a patient's stroke risk
• Ischemic stroke
• Intracranial stenosis/ blockage of the blood vessels
• Cerebral microemboli
PART 2: VERIFYING SIGNS OF COVID-19 STROKE THROUGH IMAGING
By: Robert L. Bard, MD and Dr. Pierre Kory, MD
Early detection and prevention of arterial and venous disease is key to minimizing the effects of arterial obstruction & hemorrhage, brain aneurysms, and strokes from venous thrombosis. The association of trauma to PTSD is now followed by advanced Doppler ultrasound and functional MRI. This abnormal physiology may also manifest as arterial dissection, collagen disease, inflammatory arthritis, dermatitis, ocular disorders, GI disturbances, limb pain, aneurysms of the brain and aorta. Devastating strokes in the Covid-19 era occur in the younger age group and the Latin population who are at higher risk.
INTRODUCTION
Interest in arteritis was elevated with the study of Tayakasu’s disease in the 1970's when advances in contrast arteriography diagnosed diffuse vascular involvement causing strokes and aneurysms in multiple sites. While this arterial inflammation is more common in Asians, in the US, blacks are nearly three times more likely to have a stroke at age 45 than whites. The pediatric population seems to be at higher risk for this arteritis as evidenced by their unusual rate of Covid-19 affliction affecting the vasculature and called “MULTIPLE ACUTE INFLAMMATORY SYNDROME“. Birth control pills is a distinct cause of such disease in younger women while cancer, alcoholism and obesity raise the incidence at all ages. [3]
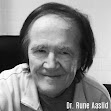
We have learned over the last century that blockages of coronary arteries to the heart and carotid arteries to the brain are precipitated by inflammation of the inner walls of the vessel, called the “intima”
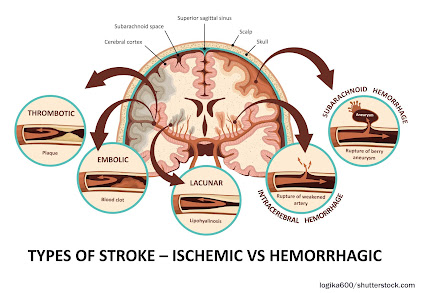
While thickening of the interior wall of vessels gradually occurs over time and is aggravated by diet, stress and hypertension (high blood pressure), the acutely disabling event occurs when there is an abrupt tear of the overlying plaque which ruptures debris which then forms a blood clot which blocks blood flow or the clot travels deeper into the brain and blocks blood flow. Similarly, abnormal heart rhythms such as “atrial fibrillation”, causes the pooling of blood in the heart which predisposes to clot formation and the clots can then travel into the brain causing a stroke. In Covid-19, the virus causing severe inflammation in the blood which then promotes clot formation which can travel through the vascular system and affect almost every organ system in the human body, with the brain and lungs being the most vulnerable. An article in September NEUROLOGY reported by Medscape documented the incidence of large artery stroke as the presenting symptom of COVId-19 was highest in men under the age of 50 years. [4]
HISTORY
A medical research team at Metropolitan Hospital in New York first noticed unusual neurologic symptoms in young and middle aged patients in the late 1960s. As a division of the NY Medical College system, they were fortunate to have an active interventional radiology department specializing in neuroimaging and arteriography. The observation of distortion and occlusion of arteries supplying the brain, kidneys, GI tract and lower limbs to various degrees from single to multiple locations was closely linked to the Japanese disorder known as Tayakasu’s arteritis at the time and recently renamed “arteritis.” A clinical finding of this arterial inflammation in the abdominal aorta was pain in the upper abdomen by the great vessels by palpation. Astute physicians were successfully treating this with commonly available “aspirin.”
However, the chronic and diffuse nature of arteritis often weakened the vessel wall producing aneurysmal dilation and rupture. Today we find sophisticated non-invasive or minimally invasive modalities to be the first line of interrogation of vasculitis. [5]

COVID AND STROKE
COVID-19 was rapidly understood as a disease caused by severe and widespread inflammation and “hypercoagulability” (a tendency to spontaneously form clots in the blood vessels.) Autopsies have revealed extensive small vessel strokes, with such strokes often occurring despite aggressive blood thinner treatment and regardless of the timing of the disease course, suggesting that it plays a role very early in the disease process. In one autopsy series, there was a widespread presence of small clots with acute stroke observed in over 25%. In a recent review of the incidence of stroke in COVID-19, almost 2% of all hospital patients suffered a stroke, which is 8x higher than in patients with influenza. More worrisome is that this is almost definitely a gross underestimate given the many likely missed strokes in patients who died on ventilators who were too ill to obtain imaging, the general restrictions on and lack of autopsies, and the well-recognized decrease in the number of patients with acute stroke symptoms seeking medical attention in the COVID-19 era. Another worrisome finding from a recent study of COVID-19 cases found that 45.5% of patients reported neurologic symptoms [6,7]. This under-recognized epidemic of neurological symptoms and strokes in COVId-19 highlights the need for more intensive imaging and investigation to achieve not only earlier recognition and improved treatment of patients but in furthering understanding of COVID-19 effects on brain function.
DIAGNOSIS BY IMAGING
Blood flow abnormalities in the arterial system are best study by Doppler imaging like the weather Doppler showing tornadoes. Multiple options exist for blood flow analysis including:
- Carotid Sonogram
- Carotid Doppler
- Eye Sonography
- Transorbital Doppler
- Contrast Enhanced Ultrasound
- Transcranial Doppler
- Hybrid Imaging |
- 3D/4D Vessel Density Histogram
- Endoarterial 3D Doppler
- Retinal OCT
- Soft Tissue OCT
- Reflectance Confocal Microscopy
- Small Coil MRI
- 7 Tesla MRI |
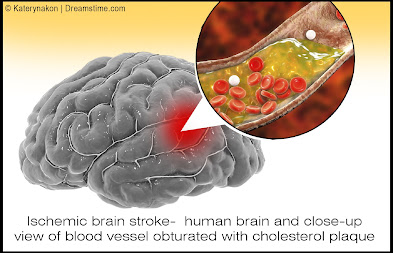
CAROTID SONOGRAM: While cerebrovascular disease is often diagnosed ex post facto after a catastrophic episode with MRI and CT, the non invasive Doppler analysis of the vascularity is generally checked with ultrasound for plaque and obstruction. A useful measure of the risk of coronary and cerebrovascular disorder is the carotid intimal thickness (CIMT). Standard depth of the inner wall thickness is a measure best obtained by high resolution sonograms since a reading over 0.9mm indicates increased risk. The newer sonogram units have depth resolution of 0.02mm making this a preferred non invasive option.
DOPPLER IMAGING TECHNOLOGIES
- COLOR DOPPLER - most common application where red is flow towards the probe and blue is flow away from the probe - POWER DOPPLER - higher spatial resolution without directional flow correlation - 3D POWER DOPPLER - allows volumetric analysis of vessel density used in treatment correlation where more vessels means increased neovascularity and fewer vessels correlates with clinical improvement - ANGIODOPPLER – similar to color Doppler with higher spatial resolution - MICROVASCULAR DOPPLER-images capillary flow - B-FLOW DOPPLER-not true flow technology but observes motion of red blood cells directly
CAROTID DOPPLER: Flow abnormalities of turbulence and absence are commonly evaluated with this modality. Plaque forms more readily in aberrant flow patterns and high velocity regions accompanying narrowing.
EYE SONOGRAPHY: Sonofluoroscopy of the orbital soft tissues and eyes is performed in multiple scan planes with varying transducer configurations and frequencies. Power and color Doppler use angle 0 and PRF at 0.9 at optic nerve head. 3D imaging of optic nerve and carotid, central retinal arteries and superficial posterior ciliary arteries performed in erect position before and after verbal communication. Retinal arterial flow is measured. Optic nerve head bulging is checked as increased intracranial pressure may be demonstrable.
TRANSORBITAL DOPPLER: R/L ciliary arteries have normal Doppler flows of 10cm/s which is symmetric.
CONTRAST ENHANCED ULTRASOUND: Widely used European nonionic contrast injection allows imaging capillary size vessels and perfusion characteristics
TRANSCRANIAL DOPPLER: This measures the flow in the anterior, middle and posterior cerebral arteries as well as Circle of Willis.
3D/4D VESSEL DENSITY HISTOGRAM: Multiple image restoration and reconstruction shows retinal vessel density of 25% at the optic nerve head and adjacent region with quantitative accuracy.[8]
ENDOARTERIAL 3D DOPPLER: Microcatheters inserted into the arterial or venous system provide measurement of wall thickness and presence of inflammatory vessels inside the intima.
RETINAL OCT: Subtraction techniques done with OCT optical coherence tomography may show changes in the caliber of the retinal vessels with verbal ideation.
SOFT TISSUE OCT: The depth of penetration may be extended to 2-3mm allowing for analysis of vascular changes in erythematous or erythropoor dermal areas. Thrombosis may be observed.
REFLECTANCE CONFOCAL MICROSCOPY: This microscopic analysis of the cells also quantifies microvascular pathology and is a potential modality for studying vasculitis.
SMALL COIL MRI: High resolution systems used for animal study and superficial organs can image the intra-arterial anatomy including dynamic contrast imaging on standard 1.5T and 3T units.
7 TESLA MRI: High field systems analyze signal abnormalites rapidly with high resolution.
HYBRID IMAGING: Hybrid imaging refers to combining diagnostic modalities to assess disease and monitor therapy.
|
Disclaimer: The information (including, but not limited to text, graphics, images and other material) contained in this article is for informational purposes only. No material on this site is intended to be a substitute for professional medical advice or scientific claims. Furthermore, any/all contributors (both medical and non-medical) featured in this article are presenting only ANECDOTAL findings pertaining to the effects and performance of the products/technologies being reviewed - and are not offering clinical data or medical recommendations in any way. Always seek the advice of your physician or other qualified health care provider with any questions you may have regarding a medical condition or treatment and before undertaking a new health care regimen, never disregard professional medical advice or delay in seeking it because of something you read on this page, article, blog or website.
REFERENCES
1) Hemodynamics: https://en.wikipedia.org/wiki/Hemodynamics
2) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5224659/
3). Hassani SN, Bard RL: Ultrasonic Diagnosis of Aortic Aneurysms. J. Natl. Med. Assoc. 66:298-299, July 1974
4). Lande A, Bard RL: Arteriography of Pedunculated Splenic Cysts. Angiology 25:617-621, October 1974
5). Lande A, Bard RL, Rossi P: Takayasu's Arteritis: A World Entity. N.Y. State J. Med. 76:1477-1482, Sep 1976
6). Helbick Eur Radiol 30:5536-5538, 2020
7). Mao l JAMA Neurol 2020 77:683-690
8). Bard RL , Gettz L, van der Bent S etal: Proceedings of the 4th Inflammatory Disease Summit at NY Academy of Medicine Nov 2021